
Discover what skin cancer staging means and its importance in treatment planning. Understand your diagnosis and boost your confidence!
What is skin cancer staging? A patient’s guide

When you hear the word “stage” attached to a skin cancer diagnosis, the instinct is to assume a universal scale from bad to worse. But skin cancer staging doesn’t work that way. What is skin cancer staging, exactly? It’s a system your dermatologist uses to measure how advanced a cancer is, whether it has spread, and what treatment makes sense, but it looks completely different depending on whether you’re dealing with melanoma, squamous cell carcinoma, or basal cell carcinoma. Understanding that distinction could change how you read your pathology report and how confidently you walk into your next appointment.
Table of Contents
- What skin cancer staging means and why it matters
- How staging varies among different skin cancer types
- Understanding melanoma staging: key measurements and stages
- Staging basal cell and squamous cell carcinomas: location matters
- What skin cancer staging means for your treatment and prognosis
- Reconsidering skin cancer staging: what patients often misunderstand
- Find expert skin cancer care and staging guidance at Rao Dermatology
- Frequently asked questions
Key Takeaways
| Point | Details |
|---|---|
| Staging defines cancer spread | Skin cancer staging shows tumor size and whether cancer has spread to lymph nodes or other parts of the body. |
| Staging varies by cancer type | Melanoma, squamous cell, and Merkel cell cancers require detailed staging; basal cell carcinoma usually does not. |
| Melanoma staging uses Breslow depth | The thickness of melanoma measured in millimeters is critical for predicting spread risk and guides staging. |
| Location impacts non-melanoma staging | Basal and squamous cell carcinoma staging applies mainly to cancers on the head, neck, or eyelid. |
| Staging guides treatment choices | Knowing your stage helps doctors choose surgery, additional tests, or systemic treatments and estimate outcomes. |
What skin cancer staging means and why it matters
Skin cancer staging describes how advanced a cancer is and whether it has spread to nearby lymph nodes or distant organs. It gives doctors a shared language to communicate about your diagnosis and a roadmap for choosing treatment. Without staging, there’s no reliable way to know whether a tumor needs surgery alone or something much more involved.
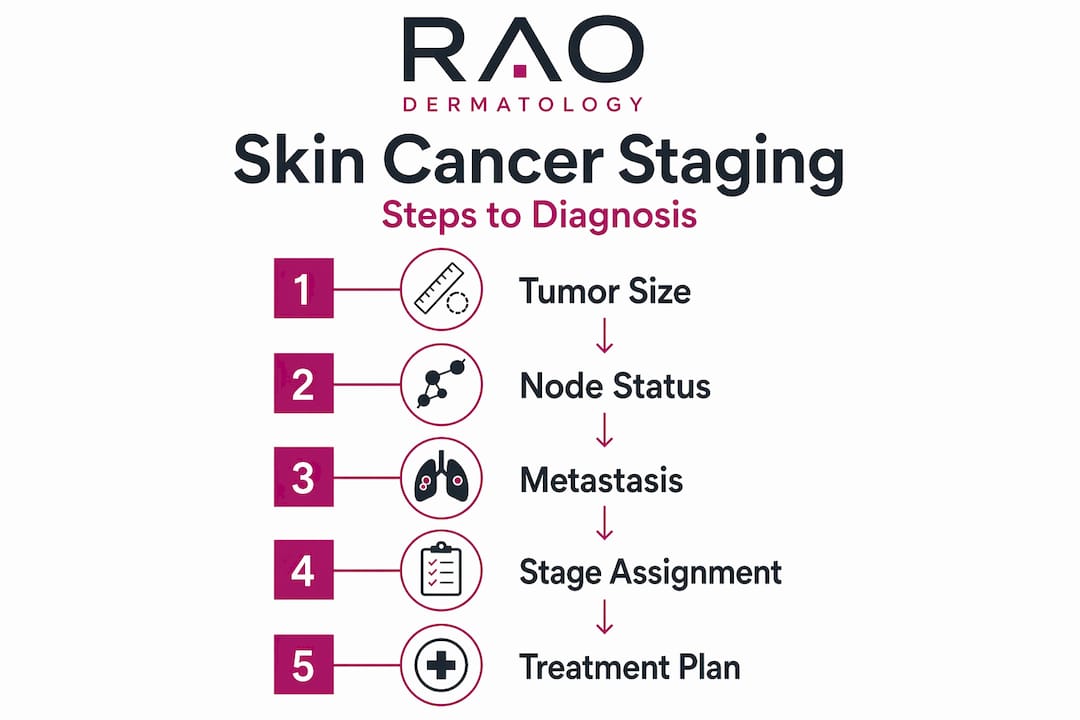
The backbone of the skin cancer staging process is the TNM system. Each letter represents a different measurement:
- T (Tumor): The size of the primary tumor and how deeply it has grown into surrounding tissue
- N (Nodes): Whether the cancer has reached nearby lymph nodes
- M (Metastasis): Whether the cancer has spread to distant parts of the body, like the lungs or liver
“Staging helps doctors understand not just where the cancer is, but where it might be going — and that makes all the difference when choosing between a simple excision and a systemic treatment plan.”
Once the TNM values are assigned, they combine into an overall stage from 0 to IV. Stage 0 means the cancer is confined to the top layer of skin, what doctors call “in situ.” Stage IV means it has spread to distant organs. Higher stages don’t just signal more risk; they signal a fundamentally different kind of clinical conversation.
Understanding skin cancer levels early also connects directly to early detection and prevention. The earlier staging occurs, the more treatment options remain available and the better the outcomes tend to be.
How staging varies among different skin cancer types
Here’s where most patients get tripped up. When you learn the skin cancer stages explained for one cancer type, you can’t assume those rules apply to another. Staging isn’t one system. It’s a family of systems.
Basal cell carcinoma (BCC) is the most common skin cancer in the US, but it rarely requires staging because it almost never spreads to lymph nodes or distant organs. Your doctor will treat it, but they likely won’t formally stage it.
Squamous cell carcinoma (SCC) is a different story. It carries a real risk of spreading, especially in immunocompromised patients or when tumors are large or located on the face. Staging matters here.
Melanoma has its own detailed, separate staging system because of how aggressively it can spread and how much fine-grained detail determines prognosis. We’ll cover this in depth in the next section.
Merkel cell carcinoma is rare but aggressive. It requires thorough staging because of its tendency to spread to lymph nodes quickly.
| Cancer type | Staging required? | Key staging criteria |
|---|---|---|
| Basal cell carcinoma | Rarely | Head/neck location only |
| Squamous cell carcinoma | Yes (often) | Location, depth, node involvement |
| Melanoma | Always | Breslow depth, ulceration, nodes |
| Merkel cell carcinoma | Yes | Tumor size, node involvement |
One detail most patients miss: staging for BCC and SCC depends on where on the body the cancer appears. Head and neck tumors are staged differently from eyelid tumors, and cancers on the trunk or extremities often have no formal staging at all. Location isn’t just context. It’s part of the classification itself.
Learn more about how skin cancer types differ in risk and presentation to put staging in fuller context.

Pro Tip: Ask your dermatologist specifically which staging system applies to your cancer type and location. “What stage am I?” is only half the question. “Which staging system are you using?” is the other half.
Understanding melanoma staging: key measurements and stages
Melanoma staging is the most detailed of all the skin cancer classification systems. It’s driven by two physical measurements taken from the excised tumor and assessed under a microscope.
- Breslow depth: The tumor thickness in millimeters measured from the top layer of skin down to the deepest cancer cell. A tumor measuring 0.5 mm is very different from one measuring 3.0 mm. This single measurement is arguably the most important number in your melanoma diagnosis.
- Ulceration: When the overlying skin has broken down over the tumor, it signals more aggressive behavior. Ulceration automatically pushes a melanoma into a higher risk category even without changing the Breslow depth.
- Mitotic rate: How fast the cancer cells are dividing, though this plays a larger role in early-stage tumors.
- Lymph node involvement: Confirmed spread to nearby nodes moves the diagnosis to stage III.
- Distant spread: Any metastasis to organs or distant lymph nodes defines stage IV melanoma.
| Stage | Breslow depth | Ulceration | Node involvement | Distant spread |
|---|---|---|---|---|
| 0 (in situ) | Confined to epidermis | None | None | None |
| I | Up to 2.0 mm | Absent (IA) or present (IB) | None | None |
| II | Greater than 2.0 mm | Variable | None | None |
| III | Any | Any | Yes | None |
| IV | Any | Any | Any | Yes |
Sub-staging matters more in melanoma than in most cancers. The difference between stage IA and stage IB isn’t just a letter. It can determine whether a sentinel lymph node biopsy is recommended or whether you need imaging. Each sub-stage maps to a specific clinical protocol.
Pro Tip: If you receive a melanoma diagnosis, ask your pathologist’s report specifically for the Breslow depth in millimeters and whether ulceration is noted. These two values will shape nearly every decision that follows.
Learn the foundational concepts behind melanoma staging and diagnosis before your next consultation.
Staging basal cell and squamous cell carcinomas: location matters
When people search “what are skin cancer stages,” they’re often asking about BCC and SCC since those are by far the most common diagnoses. The answer is genuinely more complex than most online resources acknowledge.
For BCC and SCC on the head and neck, a formal staging system applies. Stages run from 0 to IV:
- Stage 0: Carcinoma in situ, cancer cells present but not invasive
- Stage I: Tumor up to 2 cm, confined to skin
- Stage II: Tumor larger than 2 cm, still localized
- Stage III: Tumor has grown into deeper structures or spread to one nearby lymph node
- Stage IV: Spread to multiple nodes, distant organs, or major structures like bone
For BCC and SCC on the eyelid, a completely separate staging system exists. It accounts for the delicate anatomy and different spread patterns in that region.
For BCC and SCC anywhere else on the body, including the back, arms, and legs, no formal staging system applies. That doesn’t mean the cancer is ignored. It means the dermatologist focuses on tumor characteristics like depth, perineural invasion, and margin status rather than an assigned stage number.
The staging process for these cancers involves both clinical examination and surgical pathology, meaning the tissue removed during excision tells the full story. For higher-risk SCC cases, sentinel lymph node biopsy or imaging may be added.
Treatment for these cancers, including Mohs surgery for precise removal, often happens before formal staging is fully complete in low-risk cases, because the surgery itself provides the pathological data needed to confirm the diagnosis.
What skin cancer staging means for your treatment and prognosis
Understanding skin cancer levels isn’t just academic. It has direct, practical consequences for what happens to you next.
Lower-stage cancers (stages 0 through II) are typically local disease. Treatment usually involves surgical removal, and for many patients, that’s the end of active treatment. The five-year survival rates at these stages are excellent.
Higher-stage cancers (stages III and IV) require a more complex approach:
- Sentinel lymph node biopsy to confirm or rule out lymph node spread
- Systemic therapies including targeted drugs or immunotherapy for melanoma
- Radiation for cancers with perineural involvement or unresectable disease
- PET or CT imaging to look for distant spread
- Clinical trial eligibility based on specific stage sub-classification
Staging also guides follow-up care. A patient with stage IA melanoma may need annual skin checks, while a stage III patient might have imaging every six months for several years. The stage isn’t just about today’s treatment. It shapes the surveillance plan for years ahead.
Pro Tip: Ask your care team for a written copy of your staging details, including the T, N, and M values, not just the summary stage number. That level of detail will help any specialist you see understand your case immediately.
For patients in California, New Jersey, or New York, access to a dermatologist experienced in Mohs surgery and skin cancer removal can make a meaningful difference in both accuracy and outcomes at early stages.
Reconsidering skin cancer staging: what patients often misunderstand
Here’s what 25 years of skin cancer care has taught us: the most dangerous assumption a patient makes is that all skin cancers share one universal staging system. They don’t. And that assumption leads to real confusion in exam rooms across California, New Jersey, and New York every week.
Patients often assume that a “stage I” label for squamous cell carcinoma means the same thing as “stage I” for melanoma. It doesn’t. The criteria, the risk calculations, and the treatment implications are entirely different. Treating these systems as interchangeable is like comparing a blood pressure reading to a cholesterol level because they both produce numbers.
The Breslow depth is where this confusion does the most damage. Patients sometimes hear that their melanoma is “thin” and assume that means nothing needs to happen. But a 0.8 mm melanoma with ulceration is a different clinical situation than a 0.8 mm melanoma without it. The measurement isn’t arbitrary precision. Every millimeter and every pathological feature has a direct line to your prognosis and your treatment plan.
The most empowered patients we see are the ones who walk in asking specific questions: What is my Breslow depth? Is there ulceration? What is the N classification? Those questions move the conversation from passive reception to active partnership. When you understand the skin cancer staging process in detail, you don’t just receive a plan. You participate in building one.
Consult with a specialist experienced in skin cancer carcinomas before your treatment begins. Not all providers use every staging criterion consistently, and a second opinion from a specialist can surface nuances that change your plan.
Find expert skin cancer care and staging guidance at Rao Dermatology
A skin cancer diagnosis raises immediate questions: How advanced is it? What does this stage mean for treatment? What comes next? At Rao Dermatology, our board-certified dermatologists answer those questions precisely, not in generalities.
With locations in California, New Jersey, and New York, we provide expert skin cancer diagnosis and staging backed by over 25 years of specialized experience. Whether you’re managing a new BCC diagnosis or navigating the complexities of advanced melanoma staging, our team builds a treatment plan specific to your cancer type, anatomical location, and stage classification. Explore the full range of our dermatology services or visit Rao Dermatology to schedule a consultation and take the first step toward a clear, confident understanding of your diagnosis.
Frequently asked questions
What does the TNM system stand for in skin cancer staging?
TNM stands for Tumor, Nodes, and Metastasis, measuring the size of the primary tumor, whether cancer has spread to nearby lymph nodes, and whether it has reached distant organs. Together, these three values combine into an overall stage classification.
Is staging necessary for all types of skin cancer?
No. Staging is essential for melanoma, squamous cell carcinoma, and Merkel cell carcinoma, but basal cell carcinoma is rarely staged because it almost never spreads beyond its original site.
What is Breslow depth and why is it important?
Breslow depth is the measurement of a melanoma’s thickness in millimeters from the skin surface to the deepest tumor cell, and it directly predicts spread risk and determines which melanoma stage applies.
Can basal cell carcinoma outside the head and neck be formally staged?
No. No staging system exists for basal cell carcinoma or squamous cell carcinoma occurring outside the head, neck, or eyelid regions, though tumor characteristics still guide treatment decisions.
How does skin cancer stage affect my treatment options?
Early-stage cancers are typically treated with surgery or localized therapy, while advanced stages may require lymph node assessment, systemic therapies, or imaging to detect distant spread. Staging guides both treatment and follow-up intensity for years after initial diagnosis.
Recommended
- What Is Dermatoscopy? Guide to Early Skin Cancer Detection | Rao Dermatology
- Skin cancer screening: early detection and prevention | Rao Dermatology
- Types of skin cancer: Risks, signs, and prevention explained | Rao Dermatology
- Annual Skin Cancer Screening: Your Complete Guide to Dermatology Checkups | Rao Dermatology
Filed under: