
Discover what is contact dermatitis, its causes, symptoms, and effective treatments. Get expert insights to manage your skin condition today!

Contact dermatitis is defined as inflammation of the skin triggered by direct contact with an irritant or allergen, producing a localized rash that itches, burns, or blisters. The condition splits into two distinct types: Irritant Contact Dermatitis (ICD) and Allergic Contact Dermatitis (ACD), each driven by different biological mechanisms. Patch testing and topical corticosteroids are the two most referenced clinical tools for managing it. If your skin has flared up after touching a new soap, metal jewelry, or cleaning product, you are likely dealing with one of these two forms. Understanding which type you have changes everything about how you treat it.
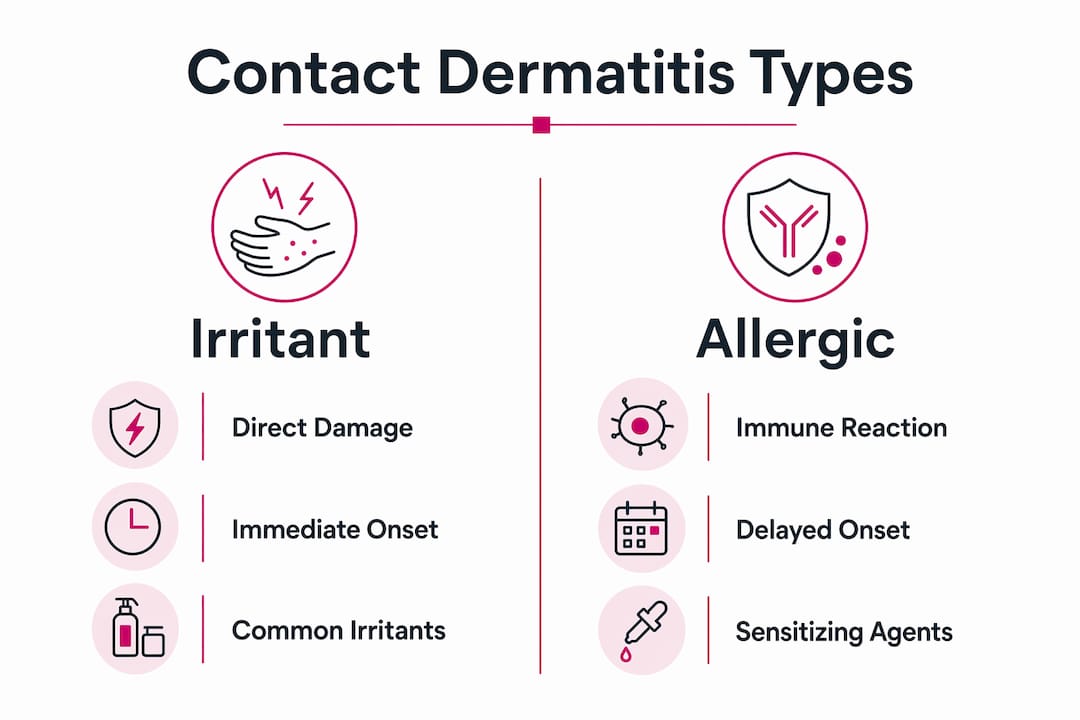
What is contact dermatitis and how do the two types differ?
Contact dermatitis is inflammation caused by two fundamentally different mechanisms, and confusing them leads to ineffective treatment. ICD results from direct chemical damage to the skin barrier. No immune system involvement is required. Common culprits include detergents, bleach, solvents, and prolonged water exposure. Healthcare workers and hairdressers develop ICD at high rates because their hands are in contact with these substances daily.
ACD, by contrast, is a T-cell mediated delayed hypersensitivity reaction. Your immune system first becomes sensitized to a substance, then mounts an attack every time it encounters that substance again. Common allergens include nickel (found in jewelry and belt buckles), fragrance compounds, latex, and preservatives like methylisothiazolinone found in many personal care products. The reaction does not happen on first exposure. It requires prior sensitization.

| Feature | Irritant Contact Dermatitis | Allergic Contact Dermatitis |
|---|---|---|
| Mechanism | Direct chemical skin damage | T-cell immune response |
| Onset | Minutes to hours after contact | 24 to 48 hours after exposure |
| Sensation | Burning or stinging | Intense itching |
| Who gets it | Anyone with enough exposure | Only sensitized individuals |
| Resolution | Improves 1 to 2 days after removal | May worsen 2 to 3 days after removal |
The timing difference matters enormously for self-diagnosis. If your skin burns immediately after touching a cleaning product, that points to ICD. If intense itching begins the day after wearing a new watch, ACD is the more likely explanation.
Pro Tip: Keep a simple log of what touched your skin in the 48 hours before a flare. This single habit gives your dermatologist the most useful diagnostic information possible.
What are the symptoms of contact dermatitis?
The symptoms of contact dermatitis range from mild redness and itching to severe blistering and open sores, depending on the substance involved and the duration of exposure. The most common signs include:
- Pruritus (itching), often intense in ACD
- Erythema (redness) at the contact site
- Swelling or edema of the affected area
- Vesicles or blisters that may weep fluid
- Scaling, flaking, or crusting as the rash resolves
- Burning or stinging sensation, more common in ICD
One critical and often overlooked point: in darker skin tones, redness may not be visible at all. Hyperpigmentation, swelling, or textural changes like scaling are the primary signs to watch for. Relying solely on redness to identify contact dermatitis leads to missed or delayed diagnoses in patients with deeper complexions.
| Symptom | ICD Timeline | ACD Timeline |
|---|---|---|
| Onset | Minutes to hours | 24 to 48 hours |
| Peak severity | Within hours of contact | 2 to 3 days after exposure |
| Resolution | 1 to 2 days post-removal | Several days to weeks |
| Primary sensation | Burning, stinging | Itching |
The rash in contact dermatitis is confined to the contact area. A rash that appears symmetrically across your body or in areas that never touched the suspected substance is unlikely to be contact dermatitis. One exception is autoeczematization, where a severe primary reaction triggers secondary skin lesions at distant sites. This is less common but can cause confusion about the original source.
Pro Tip: Photograph your rash at onset and again 48 hours later. The progression pattern, whether worsening or improving, tells your doctor as much as the rash itself.
How is contact dermatitis diagnosed?
Diagnosis starts with a detailed patient history and physical examination. Your dermatologist will ask about your occupation, hobbies, skin care products, and any recent changes in your environment or routine. This history is often more revealing than any test, because contact dermatitis causes are almost always traceable to a specific exposure.
When the allergen is unknown, patch testing is the gold standard for confirming ACD. Small amounts of common allergens are applied to the skin under adhesive panels, left in place for 48 hours, and then read at 48 and 96 hours. A positive reaction confirms delayed-type hypersensitivity to that specific substance. Raodermatology provides a detailed breakdown of what to expect in their allergy patch testing guide.
The diagnostic process for identifying triggers follows a logical sequence:
- Document all substances that contacted the affected skin in the 48 to 96 hours before the rash appeared.
- Identify any new products, materials, or environments introduced recently.
- Consult a dermatologist for clinical examination and history review.
- Undergo patch testing if ACD is suspected and the allergen is not obvious.
- Review patch test results with your dermatologist and cross-reference with your exposure history.
- Eliminate confirmed allergens from your environment and monitor for resolution.
One challenge many patients face is that sensitization can develop after years of using the same product without any problem. A moisturizer you have used for a decade can suddenly trigger ACD if your immune system becomes sensitized to one of its ingredients. This is not rare, and it is one reason why new-onset rashes deserve a fresh look at familiar products, not just new ones. For guidance on when testing makes sense, Raodermatology’s resource on when to test for allergies is worth reviewing.
How to treat contact dermatitis effectively
Trigger avoidance is the only definitive treatment for contact dermatitis. Corticosteroids reduce inflammation, but if you continue exposing your skin to the offending substance, the rash will return. Treatment without avoidance is a temporary fix at best.
The standard treatment approach combines several strategies:
- Trigger removal: Identify and eliminate the causative substance from your skin contact. Swap products, change gloves, or modify your work environment as needed.
- Topical corticosteroids: Hydrocortisone 1% is available over the counter for mild cases. Stronger prescription formulations like triamcinolone or clobetasol are used for moderate to severe reactions.
- Cool compresses: Applying a cool, damp cloth to the affected area reduces swelling and provides immediate itch relief without medication.
- Antipruritics: Calamine lotion or topical pramoxine can reduce itching between corticosteroid applications.
- Oral antihistamines: Diphenhydramine (Benadryl) or cetirizine (Zyrtec) help with sleep disruption caused by itching, though they do not directly treat the skin inflammation.
- Barrier repair: After the acute phase, moisturizers containing ceramides, such as CeraVe or Vanicream, help restore the skin barrier and reduce future sensitivity.
For over-the-counter options to manage mild symptoms, skin care and wound care products can provide accessible relief while you work on identifying the trigger. Raodermatology’s psoriasis and dermatitis services page outlines the medical management options available for more persistent cases.
Pro Tip: Complete the full course of topical corticosteroid treatment even after your skin clears. Stopping early when symptoms improve is the most common reason contact dermatitis returns within days.
Common misconceptions about contact dermatitis
The single most anxiety-producing misconception about contact dermatitis is that it is contagious. Contact dermatitis is not contagious. You cannot catch it from another person, and you cannot spread it to someone else by touching them. When a rash appears to “spread” across your own body, it reflects either delayed reactions in areas with thinner skin or the autoeczematization response described earlier, not transmission.
A second widespread misunderstanding involves the timeline of allergy development. Many patients insist a product cannot be causing their rash because they have used it for years. In reality, sensitization can occur after prolonged exposure spanning years or even decades. Your immune system can decide, without warning, that a familiar ingredient is now a threat. This is why sudden-onset reactions to long-used products are a classic presentation of ACD, not a reason to rule it out.
“Patients often arrive convinced their rash must be something exotic because their usual products are ‘fine.’ The most common allergens are the most familiar ones: fragrance, nickel, and preservatives in everyday skin care.” This clinical reality underscores why a thorough product review is the starting point of every contact dermatitis workup.
The crescendo versus decrescendo pattern is a clinical tool that helps distinguish the two types when symptoms overlap. Allergic reactions follow a crescendo pattern, worsening over two to three days even after the allergen is removed. Irritant reactions follow a decrescendo pattern, peaking quickly and then improving once the substance is gone. Knowing this pattern helps you communicate more precisely with your doctor and speeds up the diagnostic process.
Key takeaways
Contact dermatitis resolves only when the triggering substance is identified and removed. Medication manages symptoms but does not substitute for trigger avoidance.
| Point | Details |
|---|---|
| Two distinct types | ICD results from chemical damage; ACD results from an immune reaction requiring prior sensitization. |
| Symptom timing reveals type | ICD burns within hours; ACD itches intensely 24 to 48 hours after exposure and may worsen after removal. |
| Patch testing identifies allergens | Patch testing is the gold standard for confirming ACD when the trigger is not obvious. |
| Not contagious | Contact dermatitis cannot spread between people; apparent spreading reflects delayed reactions or autoeczematization. |
| Avoidance is the cure | Topical corticosteroids reduce inflammation, but the rash returns if exposure to the trigger continues. |
What 25 years of skin cases taught me about contact dermatitis
The patients who struggle most with contact dermatitis are not the ones with severe reactions. They are the ones who underestimate how long sensitization can take to develop. I have seen patients convinced their rash is from stress or diet, when the actual cause is a fragrance they have worn for 15 years. The immune system does not announce when it decides to change its response to something familiar.
The second pattern I see consistently: patients stop treatment the moment their skin looks better. Two weeks later, they are back with the same rash. Topical corticosteroids need time to fully resolve the inflammatory cycle, not just suppress visible symptoms. Completing the course is not optional.
What I find most rewarding in managing this condition is the detective work. Contact dermatitis is one of the few skin conditions where a thorough history and a well-run patch test can lead to a definitive answer and a real solution. That is not true of every skin condition. The patients who invest time in identifying their triggers, who read labels, who ask questions about workplace exposures, are the ones who achieve long-term control. Chronic skin irritation takes a real toll on quality of life. Taking it seriously from the first flare, rather than waiting for it to become severe, makes a measurable difference in outcomes.
— Krunal
Get expert care for persistent skin reactions
If your rash keeps returning despite avoiding obvious triggers, a board-certified dermatologist can make the difference between guessing and knowing.
Raodermatology offers specialized medical dermatology services across California, New Jersey, and New York, including allergy patch testing, clinical diagnosis, and personalized treatment plans for contact dermatitis. With over 25 years of experience led by Dr. Babar K. Rao, the practice combines diagnostic precision with ongoing care to help patients identify triggers and achieve lasting relief. Explore the full range of dermatology services available and take the first step toward understanding what is actually causing your skin reaction.
FAQ
What is the difference between irritant and allergic contact dermatitis?
Irritant contact dermatitis results from direct chemical damage to the skin and can affect anyone exposed to enough of the substance. Allergic contact dermatitis is an immune-mediated reaction that only occurs in individuals previously sensitized to the allergen.
How long does contact dermatitis last?
ICD typically improves within one to two days after removing the irritant. ACD can persist for several days to weeks, and symptoms may worsen for two to three days even after the allergen is removed.
Is contact dermatitis contagious?
Contact dermatitis is not contagious. It cannot spread from person to person. Apparent spreading on your own skin reflects delayed reactions or autoeczematization, not transmission.
How is contact dermatitis diagnosed?
Diagnosis is primarily clinical, based on patient history and physical examination. Patch testing is the gold standard for identifying specific allergens when ACD is suspected and the trigger is not obvious.
Can you suddenly develop contact dermatitis from a product you have used for years?
Yes. Sensitization can develop after years or even decades of exposure without any prior reaction. A product used safely for a long time can trigger ACD once the immune system becomes sensitized to one of its ingredients.
Recommended
- How Dermatologists Diagnose and Treat Skin Allergies: Expert Allergy Care | Rao Dermatology
- Atopic Dermatitis: Complete Guide to Symptoms, Causes, and Treatment Options | Rao Dermatology
- What Is Dermatitis? Symptoms, Types, and Treatment | Rao Dermatology
- Eczema: Complete Guide to Symptoms, Types, Causes, and Treatment Options | Rao Dermatology
Filed under: